Medical science is full of specialist terms, and although they’re a time-saver for those ‘in the know’, they can occasionally cause confusion! That’s the case for some of our clinical contacts, who being familiar with the long-established technique of focused ultrasound (FUS) for therapy, are sometimes unclear about how it differs from our own functional ultrasound (fUS) imaging technology.
So here we dig into the differences between the history, features and applications of these two useful ultrasound technologies – and show how they could even be used alongside each other to gain better insights into the effects of therapeutic ultrasound on the brain.
What’s the history and applications of FUS and fUS?
Let’s start by looking at how FUS and fUS were developed.
FUS is the older of the two technologies, with the first FUS device having been developed in the 1940s by researchers at the University of Illinois, USA. The focused beams of ultrasound generated by these devices were found to produce tissue lesions, which pointed towards its potential for therapeutic applications and especially tumor treatment.
Such high-intensity focused ultrasound (HIFU) technologies were investigated for several decades, but clinical applications had to wait until the development of imaging-based guiding techniques in the 1990s. The applications studied have since expanded further, and now include low-intensity focused ultrasound (LIFU) treatments that aim to stimulate or modulate certain tissue functions, rather than merely destroying the cells.
As a result of this long history in the clinic, it’s natural that when people hear mention of ultrasound in the context of the brain, they naturally think of focused ultrasound therapy rather than functional ultrasound imaging, with misunderstandings also arising from the similar abbreviations.
However, unlike FUS, fUS is a relative newcomer. The concept of using very high framerates to improve the sensitivity of Doppler-based imaging was developed in the early 2010s by researchers at ESPCI Paris, and following further research and proof-of-concept studies, some of these researchers went on to set up Iconeus in 2016.
The potential of fUS for brain imaging has grown swiftly since then, with the technique now used to investigate resting-state functional connectivity, study the responses of the brain to sensory stimulation or drugs, and to generate detailed maps of the neurovascular network. So far, all this work is preclinical, though clinical applications are in the pipeline.
How do FUS and fUS differ in how they work?
Although both FUS and fUS use ultrasound, they’re quite different in terms of their hardware and mode of operation.
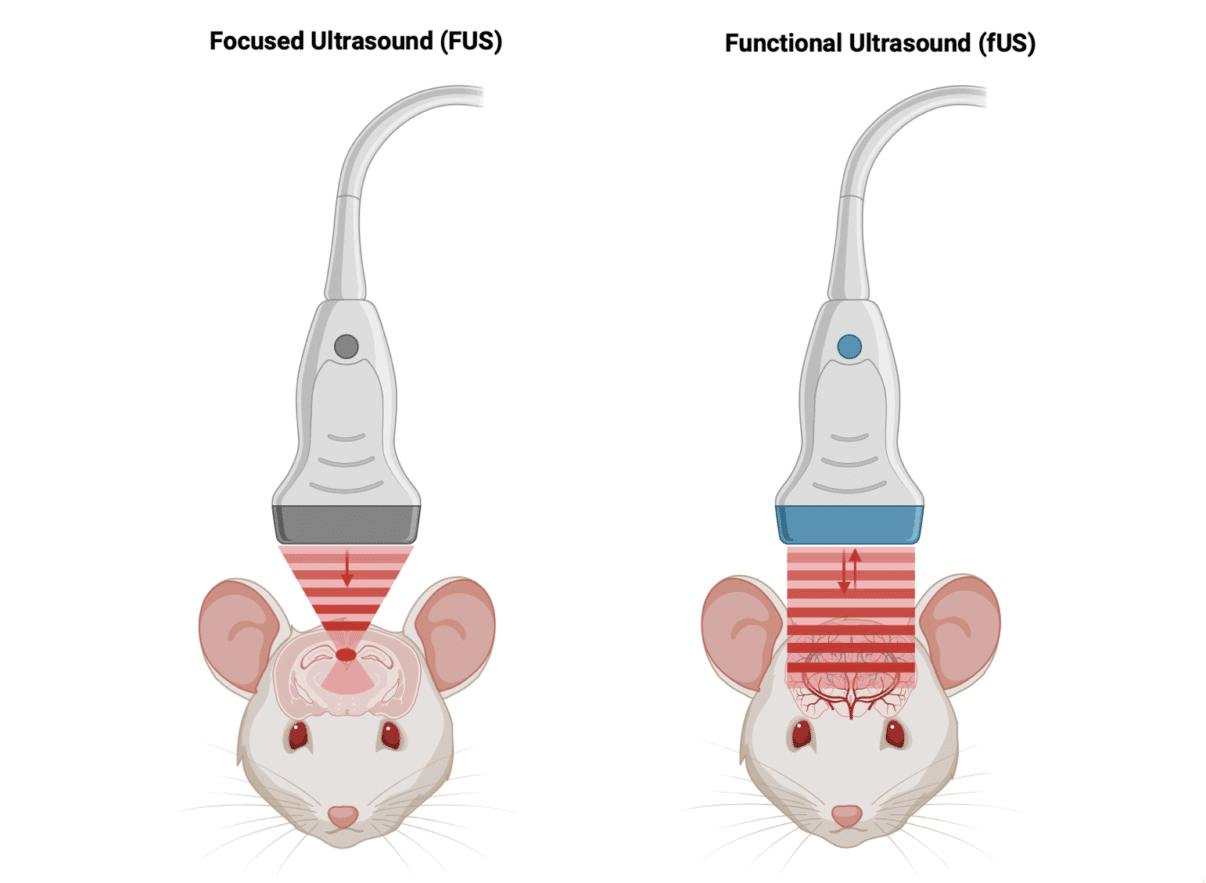
FUS uses multiple beams of relatively low-frequency ultrasound (typically within 0.2–3 MHz, depending on the target and application), which are focused on the target using mechanical or phased-signal ‘acoustic lenses’ (also known as ‘transmit focusing’). In order that the heat does not dissipate, all this energy is delivered very quickly, meaning that the effect remains localized to the target region.
Interventions targeted using FUS range across the body, including major organs, soft tissues, blood vessels, and the central and peripheral nervous systems.
In contrast, fUS uses a sequence of discrete pulses of high-frequency ultrasound (typically 15 MHz in small-animal imaging), which are usually delivered from a linear transducer array to produce a set of unfocused low-energy ‘plane-waves’ across the region of interest (termed ‘distributed insonification’). The echoes from these pulses are captured by the same transducer array, with the ultimate result being a crisp 2D or 3D image showing the blood volume distribution.
In contrast to FUS, the vast majority of applications of fUS involve the brain, where the high sensitivity of the technique provides the greatest advantage over other imaging modalities. In the brain, the principal reflectors are red blood cells – which means that fUS provides information not just on the vasculature but on neuron activity (thanks to the neurovascular coupling).
It’ll be clear from these descriptions that FUS therapy equipment cannot be used to carry out fUS imaging, and vice versa.
The lower-case ‘f’ in fUS is used by analogy to functional magnetic resonance imaging (fMRI).
FUS and fUS compared
So with the differences between FUS and fUS cleared up, here’s a table providing an at-a-glance comparison:

Combining FUS and fUS: Improving understanding of therapeutic effects
But the story of FUS and fUS doesn’t end there. Despite the long history of FUS, its use at low intensities to modulate brain functions has been hampered by the lack of in vivo studies that provide a detailed understanding of its effects as a cellular level, and especially the microscopic displacement of neuronal tissue that it induces.
This is largely down to the limitations of currently used brain imaging systems. Conventional (B-mode) ultrasound imaging suffers from limited contrast in soft tissues like the brain, while fMRI is costly and cumbersome. Moreover, imaging is normally conducted after the FUS pulse is complete, limiting the information that can be obtained on transient effects.
As those familiar with fUS will know, it provides a more information-rich imaging approach in preclinical models, by enabling high-resolution, real-time imaging of blood flows, at the same time as offering far greater operational convenience.
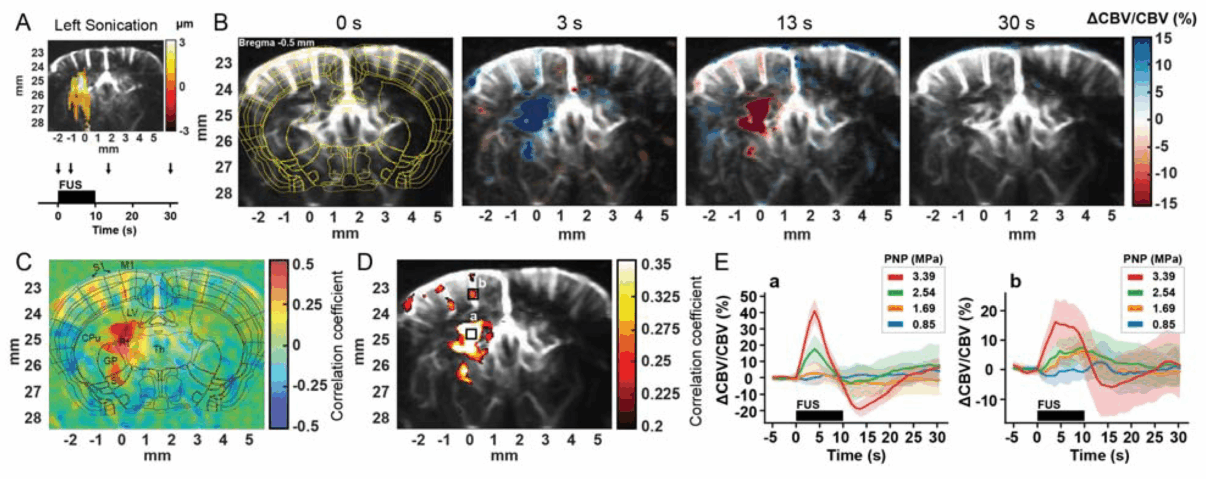
So could it be used alongside FUS? The answer is “yes”, as demonstrated in a 2024 paper [1], in which the authors generated fUS data that demonstrated correlations between FUS in the mouse brain and acoustic pressure, duration of sonication and pulse duration. As the authors say, “we anticipate that the insights developed in this study will provide more guided and effective FUS neuromodulation”.
Conclusion: Being clear about FUS and fUS
Although functional ultrasound has up to now been widely referred to as ‘fUS’ (and indeed, that’s what we call it ourselves), in the future it’s likely to be helpful to refer to it as ‘fUS imaging’ or ‘fUSI’ to be clear about how it differs from FUS therapy.
Making that distinction is going to be needed as the multiple roles of ultrasound in medical science become better understood by researchers and clinical practitioners. And of course it will be essential if the simultaneous use of FUS and fUS becomes more widely studied!
References
1. (a) S. Kim, N. Kwon, M.M. Hossain, J. Bendig and E.E. Konofagou, Displacement and functional ultrasound (fUS) imaging of displacement-guided focused ultrasound (FUS) neuromodulation in mice, NeuroImage, 2024, 298: 120768, https://doi.org/10.1016/j.neuroimage.2024.120768.
(b) S. Kim, N. Kwon, M.M. Hossain, J. Bendig and E.E. Konofagou, Functional ultrasound (fUS) imaging of displacement-guided focused ultrasound (FUS) neuromodulation in mice, BioRxiv (preprint), 2024, https://www.biorxiv.org/content/10.1101/2024.03.29.587355v1.